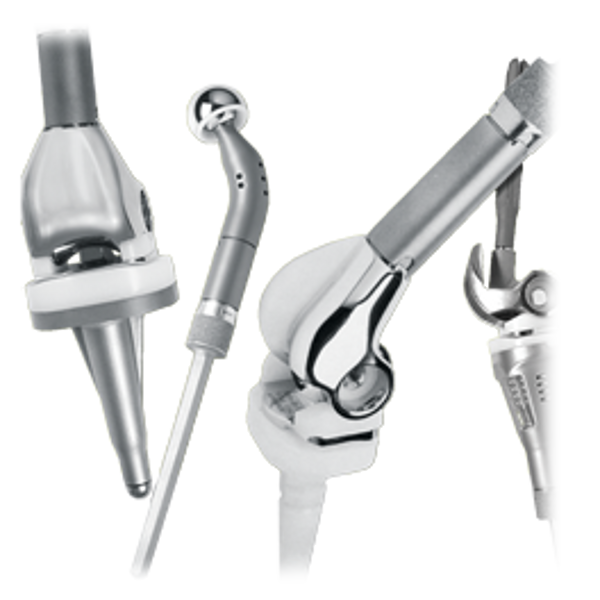
Ürün Açıklaması
ÇOK Seçenekleri Sistem diz veya kalça ağır kemik kaybı ile karşı karşıya hastaların uzuvların kullanımını yeniden sağlamak için tasarlanmıştır ve fonksiyonun restorasyonu için potansiyel sağlar.
Sistem dönen bir menteşe gereklerine ötesine geçer ve bir hastanın bireysel durumu çözmek için cerrah intraoperatif esneklik sağlar.
Anatomik, modüler ÇOK Seçenekleri Sistem maksimum intraoperatif implant seçiminde esneklik, bağlantı ve tespit verir.Sistem implant boyutları, segmentleri, adaptörler, ve bu karmaşık durumda karşılamak için kaynaklanıyor geniş bir yelpazede sunuyor.
ÇOK Seçenekleri Sistem nedeniyle ameliyat gerektiren problemleri olan hastalarda yardımcı olur:
- (Benign metastatik ve sarkom olguları dahil) Kemik tümörleri
- Aşırı kemik rezeksiyonu gerektiren Revizyon durumlarda
- Travmatik yaralanma Kemik kaybı
- Böyle osteomiyelit gibi ciddi deformite
- Ligamentöz destekleri hasar
Total Femur Bölüm bileşeni üretilmiştir Tivanium ® Ti-6Al-4V Alaşım ve veya gözenekli bir kaplama olmadan kullanılabilir.Tek bir uzunluk ve 2 oluşur ÇOK Proksimal ve Distal Femur Bileşenleri ve diğer bölümler ile kullanımını kolaylaştırmak için erkek tapers.
Segmentler Ti-6Al-4V Alaşım imal ve cerrah mümkün olduğunca yakın bacak uzunluğu geri izin vermek uzunlukları çeşitli mevcuttur. Onlar var ÇOK erkek ve bir ÇOK Proksimal ve Distal Femur Proksimal Tibia ile kullanımını kolaylaştırmak için dişi konik, ve I / M Kök Bileşenleri ve diğer bölümler.
All-Poly Patella eliptik bir şekle sahiptir ve UHMWPE üretilmiştir.
Bacak Kurtarma Cerrahi
Alt ekstremite yumuşak doku kanserlerinin tedavisi son 30 yılda önemli ölçüde geliştirmiştir. Ekstremite kurtarıcı ameliyatlar daha sık alt ekstremite tümörleri tedavi etmek için kullanılmaktadır. Geçmişte, özgün tedavi seçenekleri sınırlı ve amputasyon genellikle bu tümörlerin yönetmek için tercih seçenek oldu. Nüks ve tedavi metastaz sınırlı birçok gelişme olasılığı olasılığı.
Kemoterapi ve görüntüleme teknolojilerinde gelişmeler uzuv kurtarma tedavisi için bir kapı sağladı. Kemoterapi nüks ve metastaz ile ilişkili riskleri azaltarak yardımcı olmuştur. Bilgisayarlı tomografi (BT) görüntüleme ve manyetik rezonans görüntüleme (MRG) tümörler daha ayrıntılı ve net görüntü sağlayarak doktorlar yardım etmiş.
Diz çevresinde ekstremite kurtarılması için tasarlanmış ilk protez menteşe diz sistemleri kısıtlı idi. Bu ilk sistemler bir kapı menteşe gibi görev ve sadece ekstansiyon ve fleksiyon sağladı. Kısıtlı menteşe diz başarısı sınırlı oldu ve sık sık gevşetin olacaktır. Ayrıca, kısıtlı tasarımlar dönme stresi yönetmek ve kemik / implant arayüzünde bu stresler transfer olamazdı.Kemik / implant arayüzüne Bu gerilmeler ilk nesil menteşeli diz erken gevşeme en önemli faktörlerden biri olmuştur.
Kemik Korunması Üzerine Bir Vurgu
ÇOK Seçenekleri Sistemi ayrıca kemik implant eklemek için çeşitli seçenekler sunar. Bu seçenekler implant hastanın anatomisinin uygun başarabilen ve iyi korunan olmasını sağlamak için tasarlanmıştır. Dahil diğer önemli özelliği ÇOK Seçenekleri Sistem rezeksiyon seçenekleri bulunur. Kemik stoğu korunmuş böylece sistemi kemik koruyucu seçenekleri sağlar.
Temizleme Talimatları
Sterilite
Gama ışınlaması etiketleme sembolü ile gösterilir. Ambalaj bütünlüğü ihlal edilmemiştir gibi bu cihazlar sürece steril kalır.Kullanmadan önce her paket kontrol edin ve herhangi bir mühür veya kavite hasarlı veya ihlal veya son kullanma tarihi aşıldığında ise bileşen kullanmayın. Açıldıktan sonra bileşen kullanılması gerekir ya da atılır.
Yeniden sterilizasyon Veriler
Bu cihazlar, yeniden sterilize olabilir.
Ürün Broşürü


Indications
Contraindications
- Charcot’s joints
- Muscle deficiencies
- Multiple joint diseases
- Refusal to modify postoperative physical activities
- Obesity
- Obesity
- Heavy labor
- Active sports
- History of falls
- Use this product for other than labeled indications (off-label use)
- Use any component if damage is found or caused during setup or insertion
- Use components from other knee systems (and vice versa) unless expressly labeled for such use. Premature wear or loosening may develop and may require surgical explantation.
- Use the Tibial Revision Stem Adapter in femoral applications. It should be used only with the MOST Options Proximal Tibial Component (with or without segments).
- Impact the stem into the femoral canal after head component is assembled. Further impaction could damage the head or the Stem Adapter.
- Use the Zimmer VerSys® Hip System +10.5 Co-Cr-Mo Alloy head with the MOST Options System
- Use only the stem collet screw provided with the Hinged Femur, Hinged Tibia, and Tibial Revision Stem Adapter
- The stem collet screw has a special self-capturing feature that is designed to retain the stem should disassociation occur, and must be used with these components. No other screw should be used as a substitute
- Use only Zimmer Revision Stems of at least 190 mm in length with the MOST Options Tibial Revision Stem Adapter
- Bone screws are available for supplementary fixation as desired by the operating surgeon. These screws are not approved for attachment or fixation to the posterior elements (pedicles) of the cervical, thoracic, or lumbar spine.
- The risk of implant failure is higher with inaccurate component alignment or positioning
- Soft tissues should be balanced and components’ positioning should be confirmed
- Fat embolism risk is increased with intramedullary instrumentation and/or cement pressurization. Consider venting the femur or tibia