Product Description
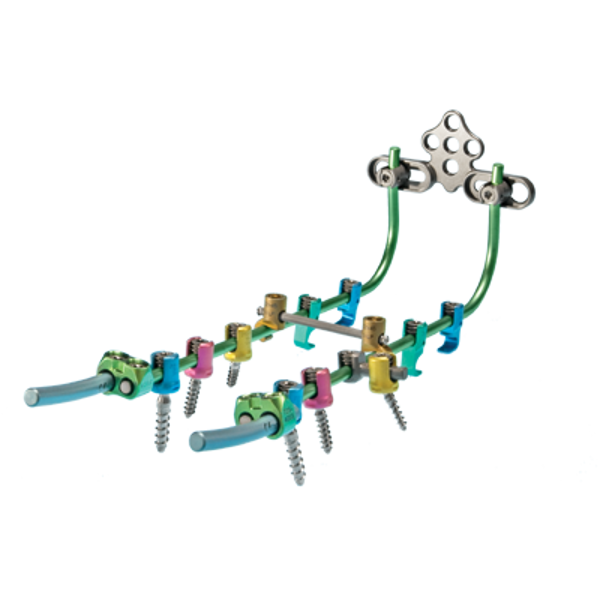
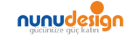
These posterior cervical spinal systems form a robust and complete posterior cervico-thoracic system. Nex-Link Spinal Fixation System and Nex-Link OCT System feature a strong occipital fixation option and a full range of screw diameters and hooks compatible with a 4.0mm diameter rod.
Features
- Robust system at any level with 4.0mm commercially pure titanium rod
- Only spinal fusion device on the market that offers full range of screw diameters (3.5; 4.0; 4.5; 5.5mm) compatible with one single rod
- Integrates adjustable occipital plate with midline fixation and pre-contoured rods
ZS-SA0700-13_A

Device Description
The Zimmer Spine Nex-Link Spinal Fixation System is intended for fixation to, and stabilization of, the cervicothoracic spine (C1-T3). The system consists of a series of longitudinal members, anchors, transverse connectors, and instruments for inserting and securing the implants.
Longitudinal members consist of 4.0 mm diameter rods manufactured from commercially pure titanium per ASTM F-67. Rods are affixed to the posterior cervicothoracic spine via anchors.
Anchors are comprised of hooks for use in the cervical and thoracic spine and screws for use in the thoracic spine. These implants are manufactured from medical grade Ti-6Al-4V ELI titanium alloy per ASTM F-136. Hooks are intended to anchor to the vertebral lamina and come in various throat depths. Screws are intended for fixation to the thoracic pedicles and are available in various diameters and lengths.
Anchors also consist of accompanying locking plugs, manufactured from medical grade Ti-6Al-4V ELI titanium alloy per ASTM F-136, to secure the rod to the hooks and/or screws.
Transverse connectors, or “cross-links”, are available to mechanically link two rods together in a construct. These implants are manufactured from medical grade Ti-6Al-4V ELI titanium alloy per ASTM F-136. Cross-links are available in various lengths to accommodate varying rod spacing.
Rod to rod connectors are manufactured from Ti-6Al-4V ELI titanium alloy per ASTM F136, and are designed to link the 4.0mm Nex-Link titanium rod to an adjacent 4.0mm or 5.5mm titanium rod.
Polyaxial offset connectors are available to mechanically link polyaxial screws to rods within a construct. These implants are manufactured from medical grade Ti-6Al-4V ELI titanium alloy per ASTM F-136.
The Zimmer Spine, Inc. Nex-Link OCT Occipital Cervical Plating System components are temporary implants that are used to stabilize the spine (occiput-T3) during the development of a solid spinal fusion in patients with degenerative disease, trauma (including fractures), and tumor pathology.
The system consists of a modular plate, rod-to-plate connectors, hooks and pre-contoured rods. Cancellous and cortical bone screws are intended for fixation to the occiput and Cannulated Side-Loading Closed Screws are intended for fixation to the upper thoracic spine.
Indications
When intended to promote fusion of the cervical spine and the thoracic spine (C1-T3), the Nex-Link Spinal Fixation System is indicated for the following: DDD (neck pain of discogenic origin with degeneration of the disc confirmed by history and radiographic studies), spondylolisthesis, spinal stenosis, fracture, dislocation, failed previous fusion, and/or tumors. Hooks and rods are also intended to provide stabilization to promote fusion following reduction of fracture/dislocation or trauma in the cervical/upper thoracic (C1-T3) spine. The use of polyaxial screws is limited to placement in T1-T3 in treating thoracic conditions only. The polyaxial screws are not intended to be placed in the cervical spine. After solid fusion occurs, these devices serve no functional purpose and should be removed. In most cases, removal is indicated because the implants are not intended to transfer or support forces developed during normal activities. The physician and the patient, taking into consideration the patient’s general medical condition and the potential risk to the patient of a second surgical procedure, must make any decision to remove the device.
The Nex-Link OCT Occipital Cervical Plating System is intended to provide stabilization as an adjunct to fusion of the cervical spine and occipito-cervicothoracic junction (occiput-T3) for the following indications: degenerative disc disease (neck pain of discogenic origin with degeneration of the disc as confirmed by patient history and radiological studies), spondylolisthesis, spinal stenosis, fracture/dislocation, atlanto-axial fracture with instability, occipito-cervical dislocation, revision of previous cervical spine fusion surgery, and tumors. The cancellous and cortical bone screws (3.5mm and 4.0mm diameters; 6.0mm-20mm threaded lengths) are used with the Nex-Link OCT System to allow for occipital fixation and limited to occipital fixation only. The Nex-Link OCT System 4.0mm cannulated side-loading closed screws are limited to placement in the upper thoracic spine (T1-T3) for additional stabilization of the cervical spine for the indications specified above.
Contraindications
The Nex-Link System is not designed or sold for any use except as indicated. DO NOT USE THE NEX-LINK SYSTEM IMPLANTS IN THE PRESENCE OF ANY CONTRAINDICATION.
Contraindications include, but are not limited to:
- Presence of overt infection and/or localized inflammation
- Rapid joint disease, bone absorption, osteopenia and/or osteoporosis
- Suspected or documented metal allergy or intolerance
- Any patient having inadequate tissue coverage over the operative site
- Any time implant utilization would interfere with anatomical structures or expedited physiological performance, such as impinging on vital structures
- Severe comminuted fractures, such that segments may not be maintained in satisfactory proximate reduction
- Use in displaced, non-reduced fractures with bone loss
- The presence of marked bone absorption or severe metabolic bone disease that could compromise the fixation achieved
- Any other medical or surgical condition that would preclude the potential benefit of surgery, such as elevation of sedimentation rate unexplained by other diseases, elevation of white blood count (WBC), fever, leukocytosis, or a marked left shift in the WBC differential count
- The physical contact of the Nex-Link System implants with metal implant made of anything other than implant grade titanium, such as stainless steel (ASTM F138) or MP35 N, or other dissimilar metal
- Situations with the absence or compromise of significant stabilizing elements
- Use in the presence of any neural or vascular deficits or other compromising pathology, which may be further injured by device intervention
- Presence of overt infection and/or localized inflammation
- Rapid joint disease, bone absorption, osteopenia and/or osteoporosis
- Suspected or documented metal allergy or intolerance
- Any patient having inadequate tissue coverage over the operative site
- Any time implant utilization would interfere with anatomical structures or expeditedphysiological performance, such as impinging on vital structures
- Severe comminuted fractures, such that segments may not be maintained in satisfactory proximate reduction
- Use in displaced, non-reduced fractures with bone loss
- The presence of marked bone absorption or severe metabolic bone disease that could compromise the fixation achieved
- Any other medical or surgical condition that would preclude the potential benefit of surgery, such as elevation of sedimentation rate unexplained by other diseases, elevation of white blood count (WBC), fever, leukocytosis or a marked left shift in the WBC differential count
- The physical contact of the Nex-Link OCT Occipital Cervical Plating System implants with metal implant made of anything other than implant grade titanium, such as stainless steel (ASTM F138) or MP35 N, or other dissimilar metal
- Situations with the absence or compromise of significant stabilizing elements
- Use in the presence of any neural or vascular deficits or other compromising pathology, which may be further injured by device intervention
Warnings
Following are specific warnings, precautions, and possible adverse events, which should be understood by the surgeon and explained to the patients. These warnings do not include all possible adverse events, which can occur with surgery in general, but are important considerations particular to metallic internal fixation devices. General surgical risks should be explained to the patient prior to surgery.
- IN THE U.S.A., THIS PRODUCT HAS LABELING LIMITATIONS.
- THIS DEVICE IS NOT CLEARED FOR SCREW ATTACHMENT OR FIXATION TO THE THORACIC (T4-T12) OR LUMBAR SPINE.
- Potential risks identified with the use of this device system, which may require additional surgery, include:
Precautions
- CORRECT HANDLING OF THE IMPLANT IS EXTREMELY IMPORTANT. Contouring of the metal implants should only be done with proper equipment. It is recommended that contouring be gradual and that great care be used to avoid any notching, scratching or reverse bending of the devices when contouring. Alterations will produce defects in surface finish and internal stresses which may become the focal point for eventual breakage of the implant.
- REMOVAL OF THE IMPLANT AFTER HEALING. Metallic implants can loosen, fracture, corrode, migrate, possibly increase the risk of infection, cause pain, or stress shield bone even after healing, particularly in young, active patients. The surgeon should carefully weigh the risk versus benefits when deciding whether to remove the implant. Implant removal should be followed by adequate postoperative management to avoid refracture. If the patient is older and has a low activity level, the surgeon may choose not to remove the implant thus eliminating the risk involved with a second surgery.
- ADEQUATELY INSTRUCT THE PATIENT. Postoperative care and the patient’s ability and willingness to follow instructions are one of the most important aspects of successful bone healing. The patient must be made aware of the limitations of the implant and follow the post-operative care regimen as instructed by his or her physician.
- DO NOT ALTER OR MODIFY ANY NEX-LINK SYSTEM INSTRUMENT. REPAIRS SHOULD ONLY BE ACCOMPLISHED BY THE MANUFACTURER. The Nex-Link System is only a temporary implant used for fixation to, and stabilization of, the cervicothoracic spine. A successful result is not achieved in every surgical case. Bone grafting must be part of the spinal fusion procedure in which the Nex-Link System is used. DO NOT ALTER OR MODIFY ANY NEX-LINK OCT OCCIPITAL CERVICAL PLATING SYSTEM INSTRUMENT. REPAIRS SHOULD ONLY BE ACCOMPLISHED BY THE MANUFACTURER. The Nex-Link OCT Occipital Cervical Plating System is only a temporary implant used for the correction and stabilization of the cervical spine. A successful result is not achieved in every surgical case. Bone grafting must be part of the spinal fusion procedure in which the Nex-Link OCT Occipital Cervical Plating System is used.
- All implants and some instruments are intended for single use only; refer to the product label to determine if the instrument is single use only. Single use devices should not be re-used. Possible risks associated with re-use of single-use devices include:
- Mechanical malfunction
- Transmission of infectious agents
- Device corrosion with localized tissue reaction and pain.
- Device migration, which may result in injury to soft tissue, visceral organs or joints.
- Loosening, or disassembly, of implant resulting in additional injury.
- Bending, loosening or breaking of the implant making removal difficult, impractical or impossible.
- Abnormal sensations, discomfort, or pain.
- Increased risk of infection.
- Bone loss due to stress shielding.
Possible Adverse Events
Occurrence of any adverse events may require re-operation and removal of the implant. Adverse events may include, but are not limited to:
- Early or late loosening of the components.
- Disassembly, fretting, loosening, bending, breakage and/or migration of any component or component portion.
- Foreign body reaction to the implants.
- Pressure on the skin from component parts where there is inadequate tissue coverage over the implant, causing skin irritation.
- Early or late infection.
- Vertebral body fracture at, above, or below the level of surgery.
- Implants cutting through bone, especially soft osteoporotic, osteopenic, or cancellous bone.
- Bone forming around the implant, making removal difficult or impossible.
- Non-union (pseudarthrosis) or bone fracture.
- Post-operative change in spinal curvature, loss of correction, height, and/or reduction.
- Neurovascular compromise including radiculopathy, paralysis, or other types of serious injury causing pain and disability.
- Hemorrhage of blood vessels.
- Soft tissue damage.
- Death.